

Heart & vascular pathology
Ischemic disease
Atherosclerotic coronary artery disease
Last author update: 11 February 2022
Last staff update: 11 February 2022
Copyright: 2014-2024, PathologyOutlines.com, Inc.
PubMed Search: Atherosclerotic coronary artery disease [title] pathology


Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Pathophysiology | Etiology | Clinical features | Diagnosis | Radiology description | Radiology images | Prognostic factors | Case reports | Treatment | Gross description | Gross images | Microscopic (histologic) description | Microscopic (histologic) images | Sample pathology report | Differential diagnosis | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Ospina-Romero M, Schulte JJ. Atherosclerotic coronary artery disease. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/heartatheroscleroticCAD.html. Accessed May 12th, 2024.
Definition / general
- Progressive luminal narrowing of coronary arteries caused by development of atheromatous plaque composed of lipids, inflammatory cells and connective tissue
Essential features
- Development of atherosclerosis follows a predictable path from initiation phase to progression and development of lipid rich atheromatous plaque to complications leading to ischemic events
- Numerous risk factors for the development of coronary artery disease are common among patients, including obesity, smoking, dyslipidemia and hypertension
- Typical atherosclerotic plaque shows a well formed necrotic core and overlying fibrous cap; smooth muscle cells, macrophages, lymphocytes, connective tissue components and calcification are variably present
Terminology
- Coronary artery disease, cardiovascular disease, myocardial ischemia, ischemic heart disease
ICD coding
Epidemiology
- Subclinical lesions may develop before adolescence; clinical manifestations commonly occur in middle aged and older adults (Diabetes Care 2014;37:2632)
- Studies suggest higher prevalence in women and higher mortality in men (Atherosclerosis 2015;241:211)
- Individuals with obesity, diabetes and hypertension
- Tobacco use
- Physical inactivity
Sites
- Coronary arteries
- Similar changes can be identified in arteries throughout the body, especially at branch points and in areas with turbulent blood flow
Pathophysiology
- Divided in 3 phases (Nat Rev Dis Primers 2019;5:56)
- Initiation:
- Deposit of cholesterol rich, low density lipoprotein (LDL) particles in the intima (fatty streak)
- Endothelial activation secondary to proinflammatory signals and mechanical stress
- Binding of LDL particles to subendothelial proteoglycans
- Aggregates engorged by smooth muscle cells (SMCs) and macrophages
- Progression:
- Recruitment of leukocytes and SMC production of extracellular matrix molecules contribute to thickening of the intimal layer
- SMCs and macrophages die, forming a necrotic lipid rich core
- Variable accumulation of calcium, large mineralization decreases risk of thrombotic event
- Complication:
- Plaque rupture: thrombus formation in plaques with large lipid core and thin fibrous cap
- Plaque erosion: plaques with rich extracellular matrix, little lipid content and thin friable fibrous cap
- Buried caps are evidence of prior rupture and healing
- Initiation:
Etiology
- At least 164 genetic risk loci have been identified (Cardiovasc Res 2018;114:1241)
- Elevated low density lipoproteins (Eur Heart J 2017;38:2459)
- Cigarette smoking (Curr Med Chem 2014;21:3936)
- Diabetes mellitus and insulin resistance (metabolic) syndrome (Endocr Rev 2019;40:1447)
- Elevated triglycerides (Arch Cardiovasc Dis 2021;114:132)
- Conditions associated with proinflammatory profile, such as systemic lupus erythematous, rheumatoid arthritis, celiac disease (Curr Opin Rheumatol 2018;30:441, Clin Rev Allergy Immunol 2020;58:1, Mayo Clin Proc 2021;96:666)
- Lifestyle and environmental factors (Eur J Prev Cardiol 2020;27:394):
- Sedentarism
- Poor diet
- Psychosocial stress
- Sleep deprivation and noise
- Certain infections (Curr Cardiol Rep 2021;23:52)
Clinical features
- Most cases remain asymptomatic for decades
- Symptoms relate to a reduction in blood flow caused by the luminal stenosis or to thrombotic obstruction (i.e. acute coronary syndrome, myocardial infarction)
- Clinical presentation can be acute or chronic and depends on the organ / body part involved
- Renovascular hypertension and reduced renal function are manifestations of atherosclerosis involving renal arteries
- References: BMC Med 2021;19:258, J Clin Med 2021;10:4664, Atherosclerosis 2021;335:31, Am J Kidney Dis 2021 Aug 9 [Epub ahead of print]
Diagnosis
- Multiple diagnostic criteria are available for symptomatic atherosclerotic lesions, depending on arterial vessel involved
- Stress tests can reveal decreased blood flow in coronary circulation
- Coronary angiography for diagnosis and therapy
- Evidence of atherosclerosis screening by imaging is limited (J Gen Intern Med 2012;27:220)
Radiology description
- Invasive angiography is gold standard to evaluate luminal stenosis
- Plaque visualization is possible with ultrasonography (US), doppler US, CT angiogram, MRI, optical coherence tomography, intravascular US (Am J Med 2009;122:S15)
- Fluorodeoxyglucose (FDG) PET evaluates plaque metabolism (Am J Med 2009;122:S15)
Radiology images
Images hosted on other servers:

Coronary angiogram

Intravascular ultrasound

Multidetector computed tomography
Prognostic factors
- Myocardial infarction, aortic dissection, abdominal aortic aneurysm and other major cardiovascular events are associated with increased mortality rates
Case reports
- 37 year old woman with heterozygous factor V Leiden mutation developed rapidly progressive angina within a month (Turk Kardiyol Dern Ars 2019;47:148)
- 53 year old man with extensive atherosclerotic lesions, Tangier disease and Leriche syndrome (J Atheroscler Thromb 2018;25:1076)
- 72 year old man with a history of coronary atherosclerosis developed left subclavian artery thrombosis compromising left internal mammary artery blood flow (Cureus 2020;12:e11524)
Treatment
- Goal is to decrease progression of atherosclerotic plaque or complications
- Low density lipoprotein cholesterol (LDL C) lowering therapy (statins)
- Antithrombotic therapy (aspirin)
- Treatment of hypertension
- Glycemic control
- Exercise
- Nutrition
- Smoking cessation
- Reference: Circulation 2019;140:e596
Gross description
- Fatty streaks are flat yellow discoloration in the intima surface
- Early plaque is raised yellow, well defined lesion, focal in distribution and irregular in shape
- Complicated plaques show ulcers, protrusions and thrombus (PLoS One 2017;12:e0186630, Arterioscler Thromb Vasc Biol 2000;20:1177)
Gross images
Images hosted on other servers:

Coronary artery atherosclerosis

Aorta involved by
atherosclerosis
Microscopic (histologic) description
- Fatty streak: subendothelial accumulation of foam cells without necrotic core or fibrous cap
- Fibrous cap atheroma (Am J Med 2009;122:S3):
- Well formed necrotic core with overlying fibrous cap; smooth muscle cells, macrophages, lymphocytes and connective tissue components may be present
- With rupture: luminal thrombus communicates with underlying necrotic core
- With erosion: luminal thrombosis; no communication of thrombosis with necrotic core
- Fibrocalcific plaque: collagen rich plaque, contains large areas of calcification with few inflammatory cells, necrotic core may be present
Microscopic (histologic) images
Contributed by Robert F. Corliss, M.D. and Jefree J. Schulte, M.D.
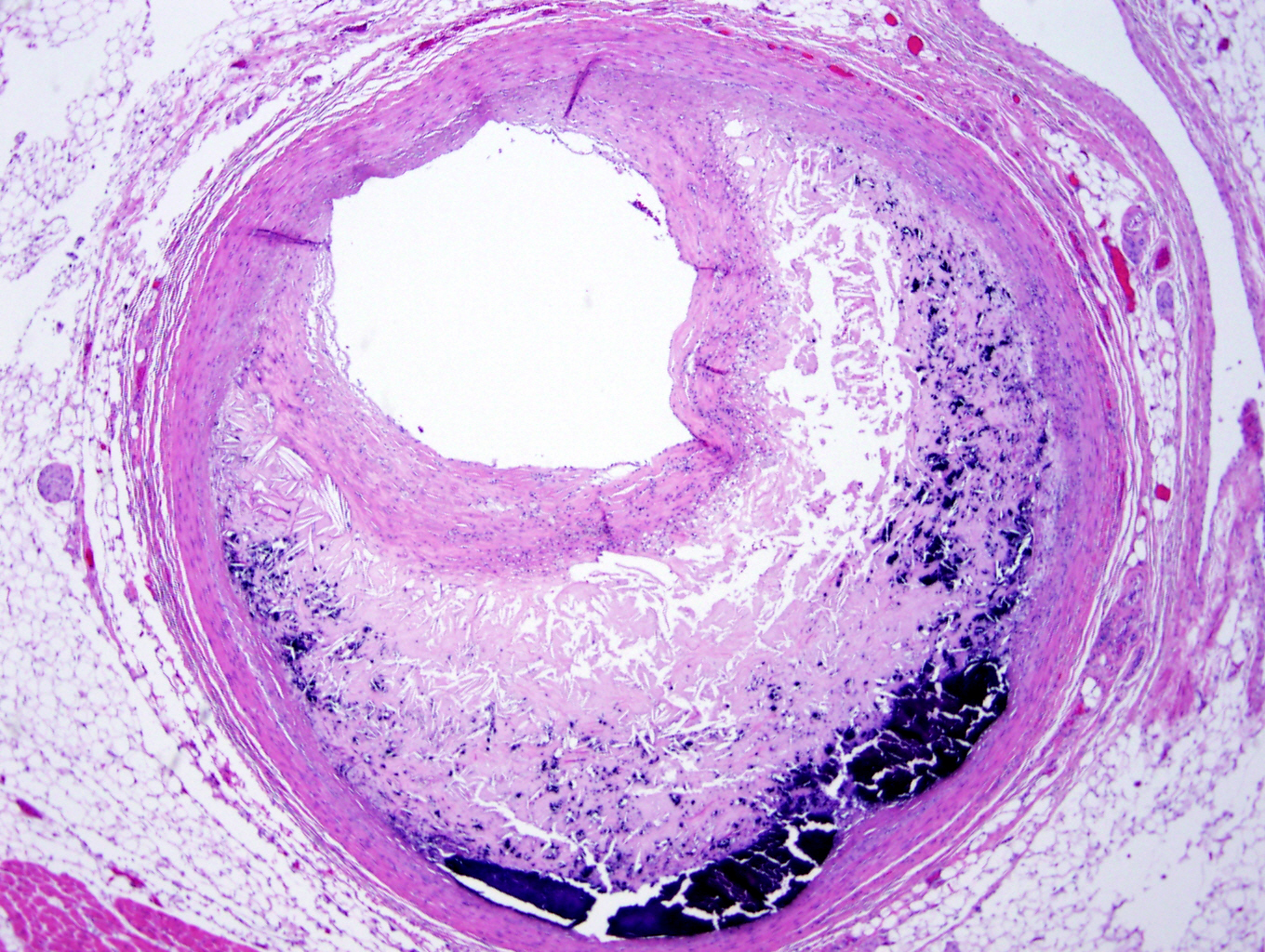
Coronary artery plaque
Coronary artery thrombus
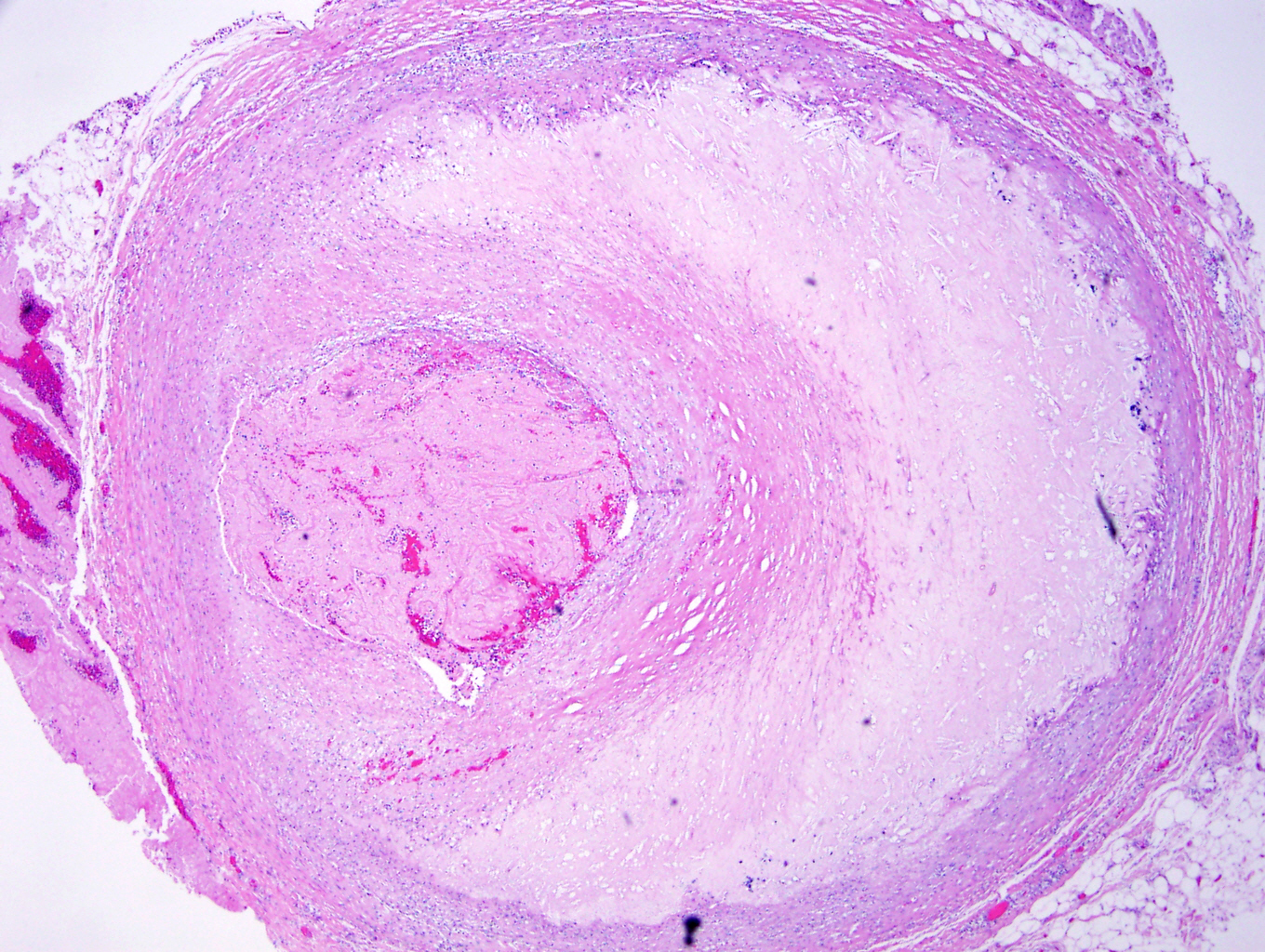
Coronary artery recanalized thrombus
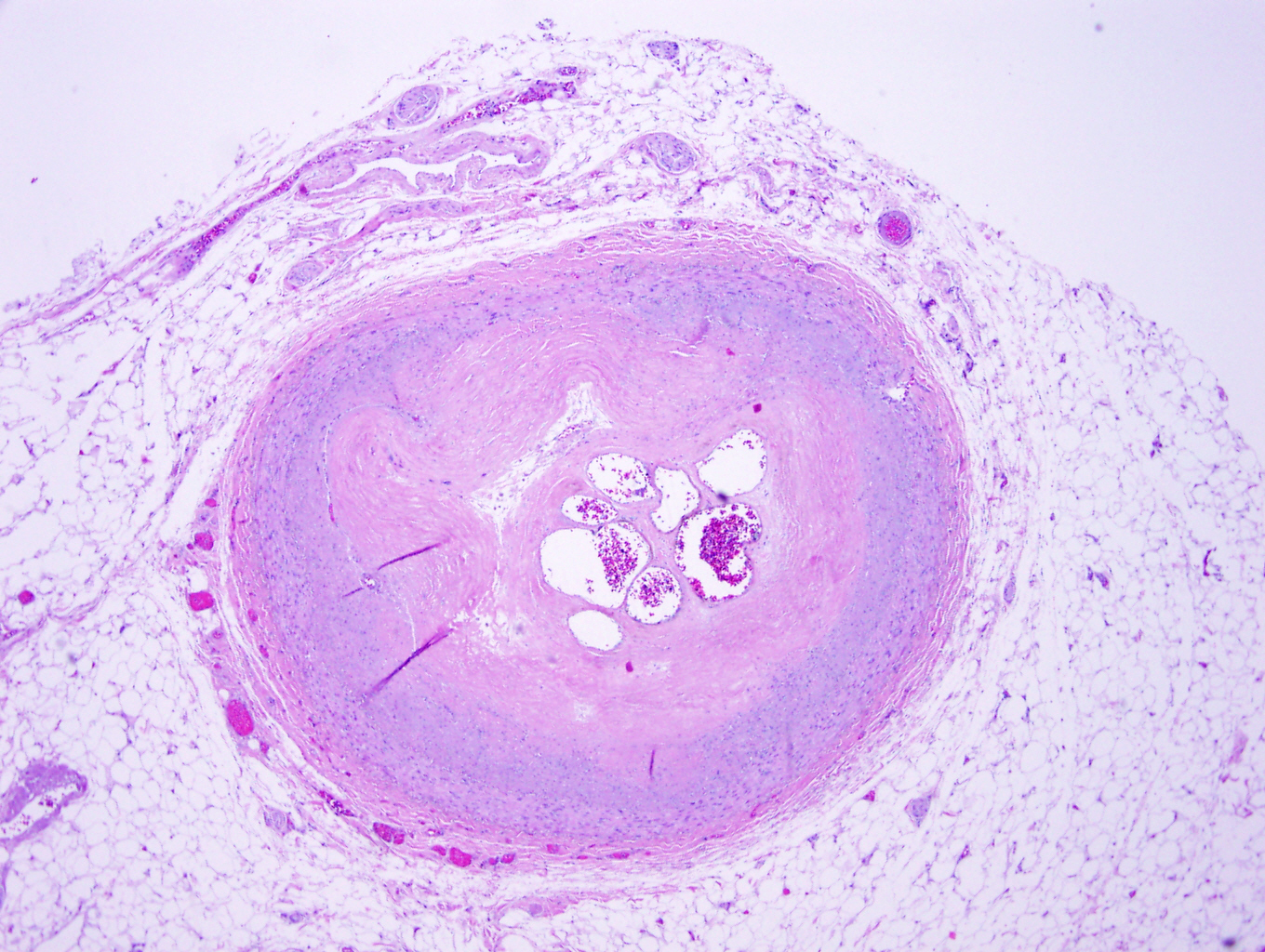
Coronary plaque with early thrombus
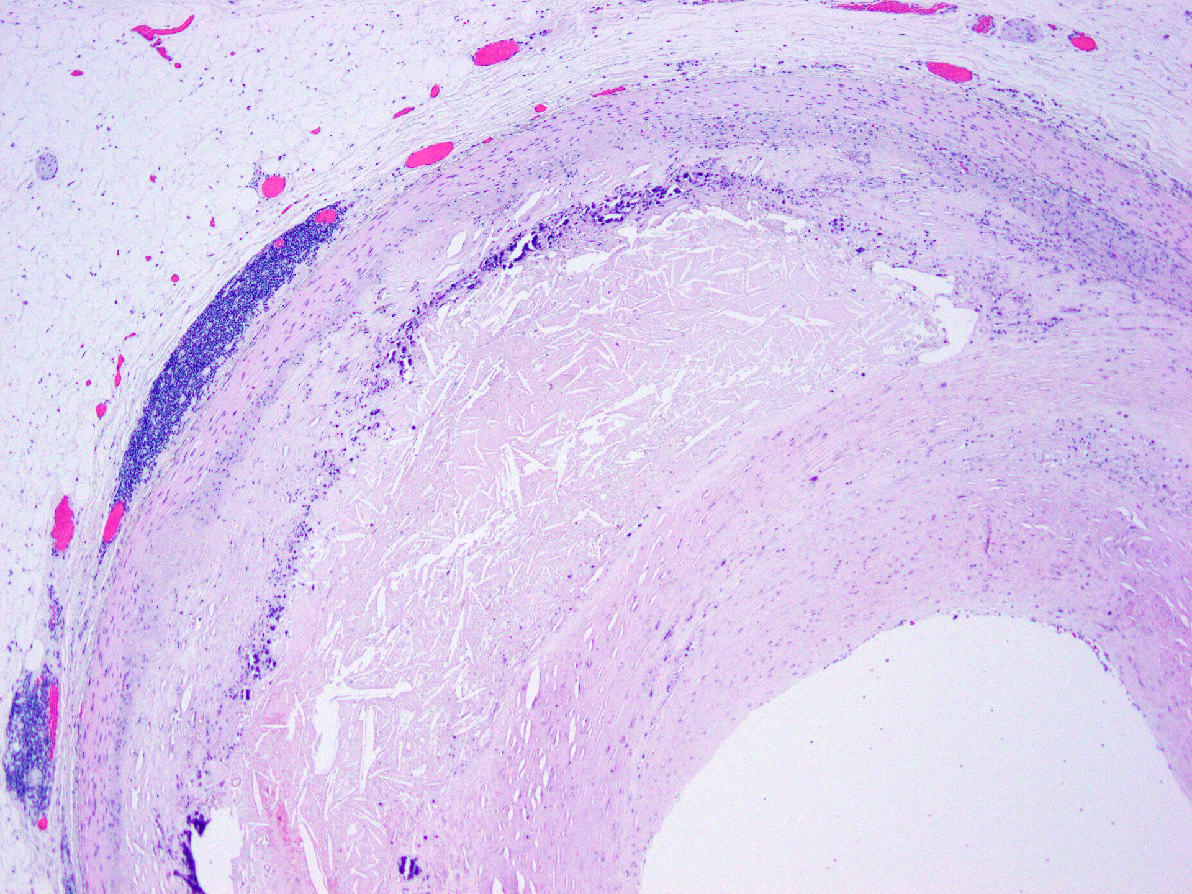
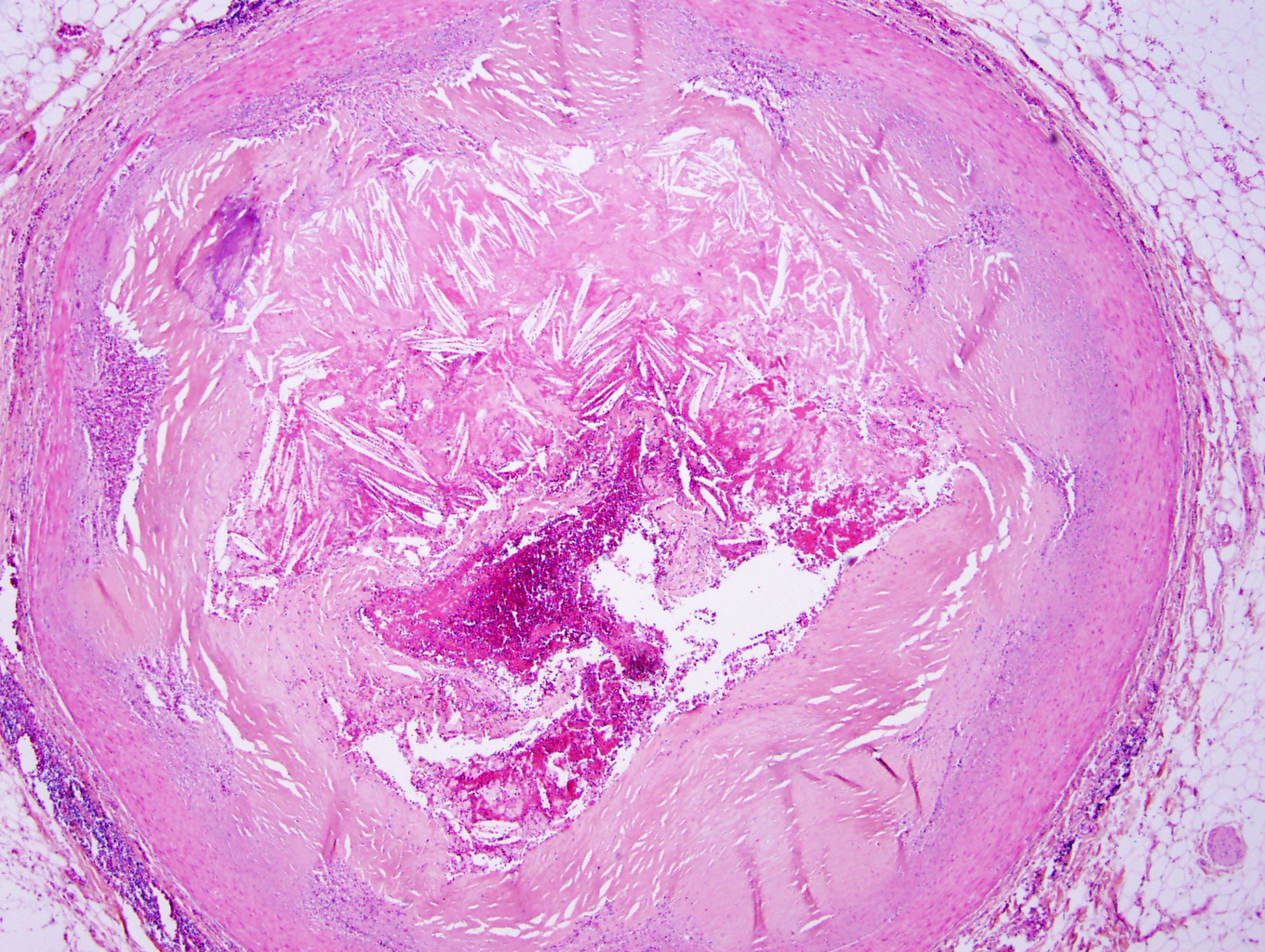
Lipid rich plaque
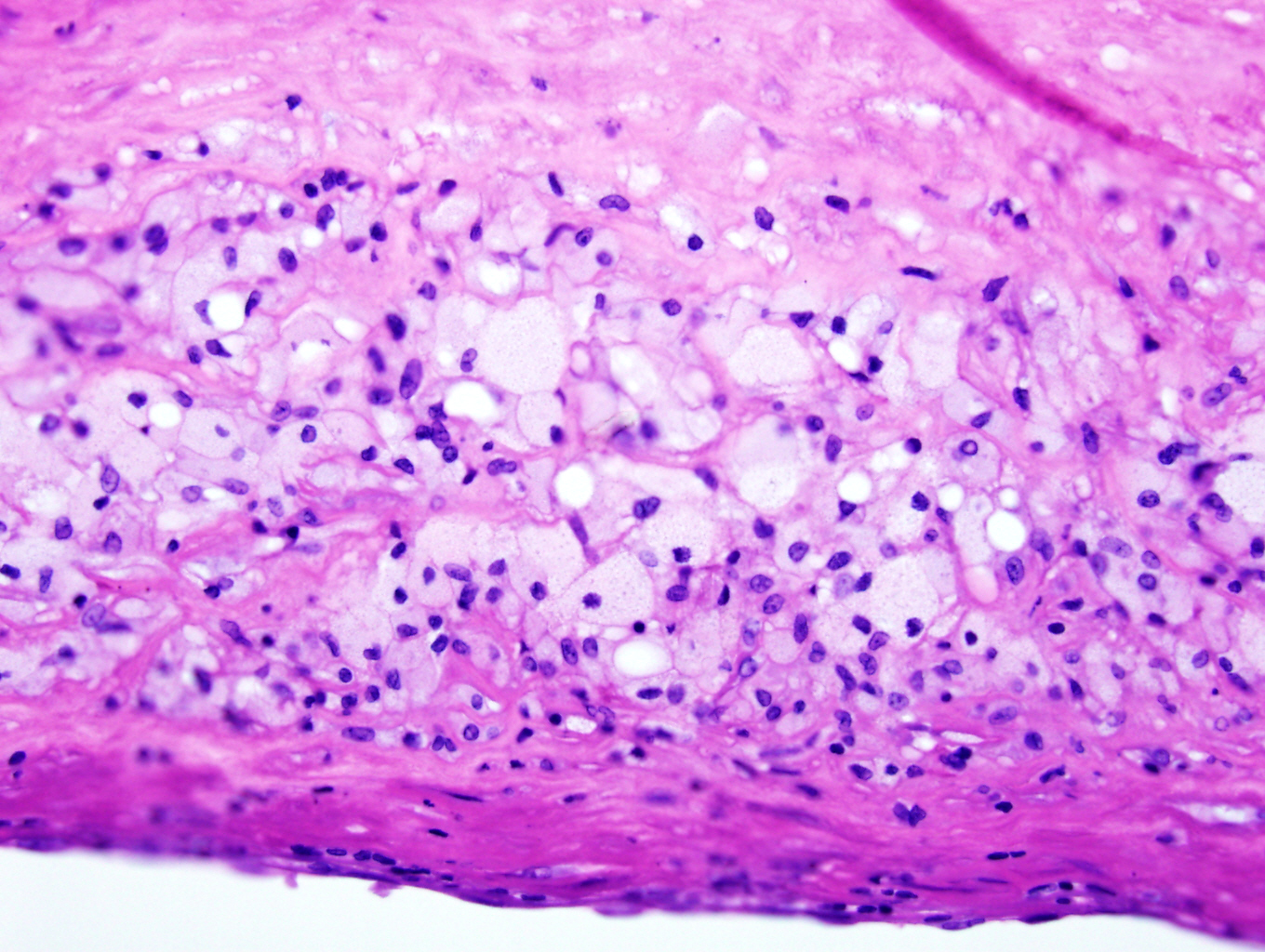
Foam cells
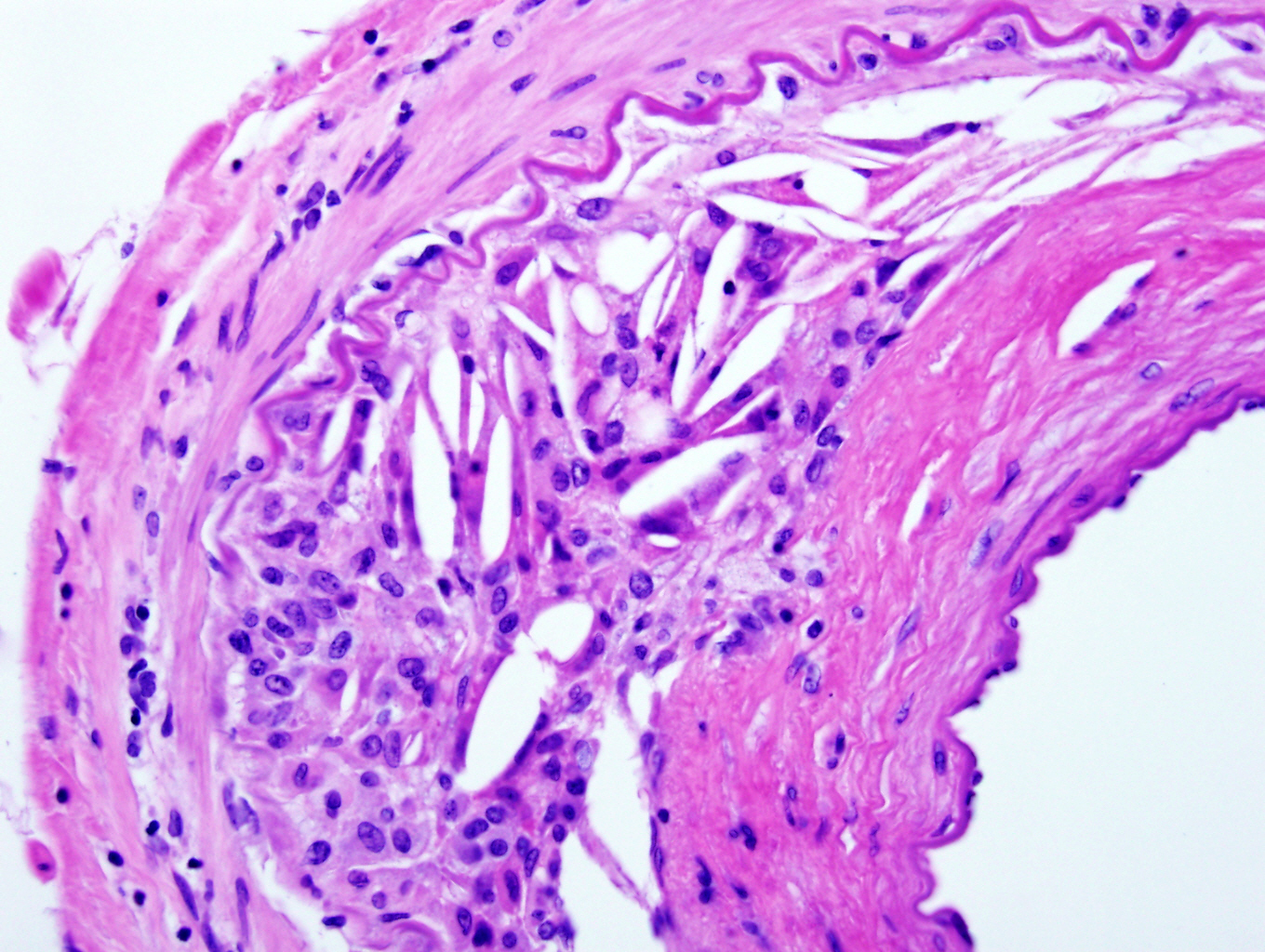
Cholesterol clefts
Sample pathology report
- Coronary arteries are not received as an anatomic pathology specimen unless part of a heart explant or autopsy case
- Heart, explant:
- Ischemic heart disease characterized by multifocal macroscopic and microscopic infarctions (weeks to months old) and severe calcific coronary artery disease
Differential diagnosis
- Coronary artery dissection or aneurysm:
- Can be seen in conjunction with coronary artery disease
- Diagnosis requires changes in vascular anatomy (separation of vessel layers in dissection and dilation of vessel in aneurysm)
- Mönckeberg medial calcific sclerosis:
- Ring-like calcification of medial layer
- Other features of atheromatous plaque are absent
- Vasculitic process:
- Often shows destruction of vessel by inflammatory infiltrate
Board review style question #1
A 75 year old man presents with acute chest pain, shortness of breath and EKG changes concerning for acute myocardial infarction. At autopsy, the above finding is identified when examining the coronary arteries. Which of the following is a risk factor for this finding?
- Coronary artery plaque with thick fibrous cap
- Lipid rich coronary artery plaque with thin fibrous cap
- Low blood triglyceride level
- Patient is a nonsmoker
Board review style answer #1
B. Lipid rich coronary artery plaque with thin fibrous cap
Comment Here
Reference: Atherosclerotic coronary artery disease
Comment Here
Reference: Atherosclerotic coronary artery disease
Board review style question #2
An adolescent male dies and undergoes autopsy. The autopsy pathologist notes some changes associated with atherosclerosis. The most likely finding to be identified at this age is
- Accumulation of calcium in vessel walls
- Fatty streak formation
- Lipid rich atheromatous plaques
- Vascular intimal thickening
Board review style answer #2
